

4/22/21 - smart, useful, science stuff about COVID-19
4/22/21 - smart, useful, science stuff about COVID-19
HAPPY EARTH DAY!

VACCINES:
1) A 4/17/21 piece by Allyson Chiu at The Washington Post offers some safekeeping tips for that white vaccination record card, if you are fortunate enough to have been vaccinated by now in the U.S. First, snap a photo of it and store the card in a safe place where you can retrieve it if necessary. Second, don’t carry it around; keep it secure, says a George Washington University Medical Faculty patient safety officer who is quoted in the piece. Third, don’t laminate the card because health care workers might add information to it later, such as any COVID-19 boosters you get, the story states. If you lose the card, return to the place where you were vaccinated (the 2nd place, if you received a 2nd dose at a different location than the 1st) and ask for a replacement. Failing that, you should be able to request a replacement from your doctor’s office or state health department, according to the deputy director of Immunization Action Coalition, a non-profit that focuses on increasing immunization rates and creates educational materials about immunizations: https://www.washingtonpost.com/lifestyle/2021/04/17/vaccine-card-record-covid-passport/.
2) The U.S. Food and Drug Administration’s 4/13/21 decision to pause the use of Johnson & Johnson’s one-shot COVID-19 vaccine in this country “has set off a chain reaction of fear” about the safety of the vaccine and is causing “unnecessary drama” during the COVID-19 vaccination campaign in the U.S., writes Sam Baker at Axios (4/14/21). The clotting issue arose in six people, one of whom died from her blood clot, among the 7 million or so people who have received the Johnson & Johnson vaccine to date, per various sources. But “of the 20 most-engaged stories on social media about the Johnson & Johnson pause, just two headlines included the context that the blood clots were rare occurrences, according to data from NewsWhip," Baker writes. Pfizer says it can increase production of its COVID-19 vaccine to help fill gaps caused by the Johnson & Johnson pause, Baker writes: https://www.axios.com/vaccine-fear-johnson-johnson-fda-887e9062-d284-48bf-9979-dc22414c2146.html.
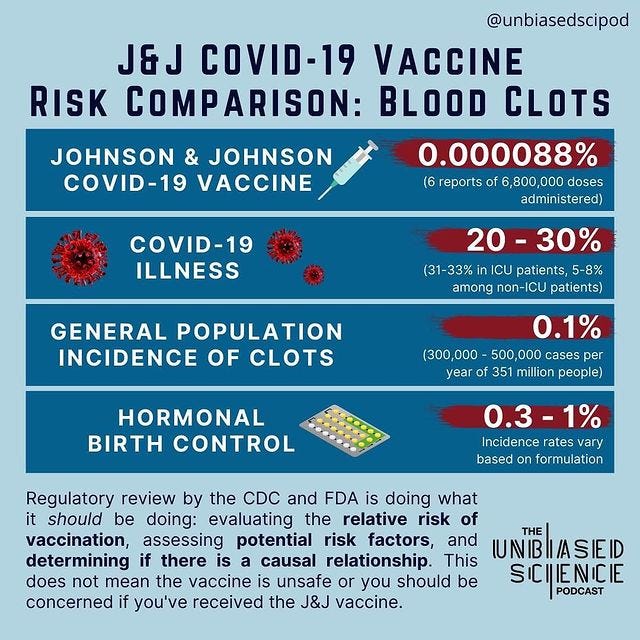
3) The Unbiased Sci Pod posted a graphic on 4/13/21 that compares the likelihood of dangerous blood clots occurring under four different scenarios or conditions — 1) the Johnson & Johnson COVID-19 vaccine, 2) having COVID-19, 3) the incidence of clots in the general U.S. population, and 4) among people taking hormonal birth control. The risk figures are 0.000088%, 20% to 30%, 0.1%, and 0.3% to 1%, respectively. Text below the graphic states, “Regulatory review by the CDC and FDA is doing what it should be doing; evaluating the relative risk of vaccination, assessing potential risk factors, and determining if there is a causal relationship. This does not mean the vaccine is unsafe or [that] you should be concerned if you’ve received the J&J vaccine”:
4) Again, it’s extremely unlikely that you would develop a clotting disorder associated with Johnson & Johnson's COVID-19 vaccine, and the benefits of the vaccine far outweigh the risks, experts say. But if you received the J&J vaccine within the past 3 weeks and have experienced headaches, abdominal pain, leg pain or shortness of breath, you should contact a health care provider, according to U.S. health agencies, writes Dr. William Petri, for The Conversation (4/13/21). The blood clots can be treated with blood thinners and anticoagulants. Currently, the U.S. Advisory Committee on Immunization Practices (ACIP), which advises the U.S. Centers for Disease Control on vaccines, is continuing to evaluate data and risks associated with the J&J vaccine. The clotting side effect has not been reported by people who received the Moderna or Pfizer COVID-19 vaccines, which rely on different technology, writes Petri, an infectious diseases specialist and immunologist at the University of Virginia School of Medicine. So, vaccination against COVID-19 continues in the U.S.: https://theconversation.com/johnson-and-johnson-vaccine-suspension-a-doctor-explains-what-this-means-for-you-158923.
5) A similar issue with dangerous blood clots has arisen with AstraZeneca’s two-dose COVID-19 vaccine, as you’ve probably heard. The incidence rate with this vaccine also is very rare, but the vaccine is now “widely accepted” to cause (not just be linked to as is currently the case for the Johnson & Johnson vaccine) dangerous blood clots and low counts of the blood component called platelets, report Kai Kupferschmidt and Gretchen Vogel at Science (4/11/21). The AstraZeneca COVID-19 vaccine is in use in the UK and the European Union, and the World Health Organization has approved its use, “allowing it to begin distribution in low- and middle-income countries,” according to this 2/19/21 Forbes story. Doses have been delivered to more than 100 countries, and the vaccine is in use in Australia, Kupferschmidt and Vogel report. “In Europe, at least 222 suspected cases of the clots and low platelet counts have been reported among 34 million people who have received their first dose” of the AstraZeneca COVID-19 vaccine, the Science story states. And “more than 30 have died,” the story adds. “In the vast majority of cases,” the benefits of the vaccine outweighs the risks, researchers agree, the story states. Researchers are trying to determine the mechanism behind the clotting issue, which resembles a rare immune-system reaction to the drug heparin, the story states: https://www.sciencemag.org/news/2021/04/hard-choices-emerge-link-between-astrazeneca-vaccine-and-rare-clotting-disorder-becomes.
6) “Concerns about blood clots with Johnson & Johnson underscore just how lucky Americans are to have the Pfizer and Moderna shots” [against COVID-19], writes Sarah Zhang at The Atlantic (4/14/21). Last year, the Moderna and Pfizer vaccine development efforts looked like long shots because they both relied on as-yet unproven messenger RNA (mRNA) technology. The Johnson & Johnson and AstraZeneca approaches looked like “medium bets” at the time, with both relying on a modified adenovirus to carry a gene with instructions for building SARS-CoV-2’s “spike protein." Now that a very small number of recipients of the J&J and AstraZeneca vaccines have suffered blood clots that might be linked to the adenovirus approach, the “risky bet” made by the U.S. on the mRNA vaccines “looks like a good one,” Zhang writes. “The unusual blood clots” have not shown up among recipients of the mRNA vaccines. However, “the rest of the world has been banking on the J&J and AstraZeneca vaccines,” Zhang writes. So "if the blood-clot risk is real…the U.S. will be fine; the rest of the world will face difficult questions about balancing the risks and benefits of an affordable, good-but-not-best vaccine against a disease that has killed nearly 3 million people” in the past year and a half, Zhang writes. Other vaccines that rely on adenovirus technology include Russia’s Sputnik V, China’s CanSino, and J&J’s Ebola vaccine, the story states. The story also describes two historical examples of how authorities have responded to vaccines for potentially dangerous diseases (polio and rotavirus) that are associated with rare cases of risky complications: https://www.theatlantic.com/health/archive/2021/04/mrna-vaccines-johnson-blood-clots/618594/.
7) The chances that you will get a “breakthrough” infection with SARS-CoV-2 despite being vaccinated more than two weeks ago (with both doses in the case of a two-dose COVID-19 vaccine) are “quite low, but not zero,” according to a 4/20/21 post at Dear Pandemic. The chances of this occurring are 0.0077%. Breakthrough infections are not surprising because some also occurred during large-scale human studies of the vaccines. A total of 95% fewer such infections occurred among study subjects who received the Pfizer COVID-19 vaccine than among subjects who didn’t, for instance, but obviously, that means some infections (8 out of 18,198 people vaccinated versus 162 in the similarly sized group of people who were not vaccinated) did break through. “The number of breakthrough infections depends heavily on the level of transmission around you — if there is very little virus circulating there is hardly any chance for you to have a breakthrough infection,” write “Those Nerdy Girls” at Dear Pandemic. So, vaccinated people should continue to avoid crowded indoor spaces and wear a mask “when you can’t avoid close contact in public,” the post states: https://dearpandemic.org/breakthrough-infections-after-vaccination/.
8) How did New Mexico became the first U.S. state to reach more than half of its adults with at least one dose of a COVID-19 vaccine, including relatively high numbers of Black, Hispanic and Asian people, despite a high poverty rate and a population with many health challenges? For starters, the state committed to a single registry for vaccine appointments, set up by the state’s health department, reports Dan Goldberg at Politico (4/12/21). In addition, the state partnered with tribal leaders and U.S. Indian Health Services to reach nearly one-third of Native Americans in New Mexico, so far, the story states. “The state’s public health challenges wound up helping speed vaccine distribution, because public health officials had so much experience dealing with communities most likely to struggle getting vaccinated,” Goldberg writes. Mobile clinics and pop-up clinics near churches helped reach homeless people and people who were undecided about vaccination, the story states. The state chose a strategy of allocating more doses to high-need communities and to reaching its elderly population, most of whom are people of color, Goldberg reports. And a centralized and concentrated health care system helped speed up progress too. The state “is now seeing fewer than 200 new infections per day, one of the lowest per capita rates in the country,” Goldberg writes: https://www.politico.com/news/2021/04/12/new-mexico-vaccines-481064.
9) I recently came across this helpful Vox video which explains clearly “why you can’t compare COVID-19 vaccines” (3/20/21): https://www.facebook.com/Vox/videos/738383430186874/.
PUBLIC HEALTH:
10) Two recent pieces explore the risks of a SARS-CoV-2 infection associated with air travel. The first one is a beautiful interactive at The New York Times that illustrates how air circulates on airplanes, though it doesn’t directly say that it illustrates how SARS-CoV-2 particles circulate in that air. The piece states that passengers constantly breath a mixture of fresh and recirculated air in most single-aisle aircraft (4/17/21). The air enters the cabin through ceiling ducts and exits through vents near the floors. “Half of the air that is sucked out is released from the plane, and the other half is filtered [by two pleated fiberglass HEPA filters] and eventually sent back into the cabin,” the piece states. The piece shows the results of some simulations it developed with researchers of how more than 2 million air particles flow in an airplane cabin and the risks posed by "infectious viral particles," including what happens to particles when someone sneezes on board. It looks like an individual’s sneeze particles stay confined within clusters of a few rows. “Air is refreshed roughly every two to three minutes — a higher rate than in grocery stores and other indoor spaces, experts say,” the piece states. “The potential risk for exposure may be just as high, if not higher, when people are in the terminal, sitting in airport restaurants and bars or going through the security line,” the piece states (By Mika Gröndahl, Tariro Mzezewa, Or Fleischer, and Jeremy White): https://www.nytimes.com/interactive/2021/04/17/travel/flying-plane-covid-19-safety.html.
11) The other air travel piece describes a recent U.S. Centers for Disease Control and Kansas State University study finding that empty middle seats can reduce the risk of a SARS-CoV-2 exposure by 23% to 57% on a single-aisle and twin-aisle aircraft, presumably compared with a full aircraft. The study simulated airborne exposure of unmasked passengers to bacteriophage particles (bacteriophages are viruses that can infect bacteria) as a stand-in for SARS-CoV-2, reports Jacqueline Howard at CNN (4/14/21). “The researchers noted that some virus aerosol can still be emitted from an infectious masked passenger and so distancing [of seats] could still be useful,” the story states. The story concludes with an update on CDC guidance for air travel: https://www.cnn.com/2021/04/14/health/airplane-seating-covid-risk-cdc-study-wellness/index.html
12) Many experts now agree that schools can re-open safely this fall if they implement coronavirus control measures including mask wearing, physical distancing of three feet with masks on and six feet with masks off (per recently updated guidelines from the U.S. Centers for Disease Control), and good ventilation, reports Tanya Lewis at Scientific American (4/15/21). As of last month, "nearly half of U.S. school campuses were open,” Lewis writes. And school reopenings in Florida, Utah and Missouri did not result in spikes in COVID-19 cases, research reveals. Studies of the effectiveness and safety of various makers’ COVID-19 vaccines in adolescents and young children are under way. Meanwhile, about 80 percent of school teachers and staffers are now fully or partially vaccinated, per the CDC, Lewis reports. “If schools require masking and do hand hygiene, the risk of mortality [for school staffers] from driving to work [and having a traffic accident] is higher for an unvaccinated adult than it is from acquiring COVID in school,” says a Duke University School of Medicine pediatrics researcher quoted in the piece. Air exchange in schools can be improved with upgrades to heating, ventilation and air-conditioning systems; opening windows; using fans; or changing air filters more frequently, the story states: https://www.scientificamerican.com/article/schools-can-open-safely-during-covid-the-latest-evidence-shows/.
13) The U.S. Centers for Disease Control (CDC) made it official on 4/5/21 — the risk of infection with SARS-CoV-2 through touching a contaminated surface is “generally considered to be low,” less than 1 in 10,000, studies show. The primary way that the virus is spread is through inhalation of tiny virus-carrying droplets in the air in unventilated spaces. Cleaning surfaces with soap and water is enough to reduce the risk of infection by this route “in most situations,” the CDC page states. The CDC announcement vindicated many scientists and writers, including Derek Thompson at The Atlantic who coined the phrase “hygiene theater” last year. The phrase described the public-health energy wasted on deep-cleaning, particularly of surfaces in public settings, energy that could be directed more effectively toward distributing masks or public health messages about social distancing. In response to the new CDC update, Thompson wrote on 4/13/21, “You can put away the bleach, cancel your recurring Amazon subscription for disinfectant wipes, and stop punishing every square inch of classroom floor, restaurant table, and train seat with high-tech antimicrobial blasts.” Yet, many businesses, schools and transit systems still engage in “hygiene theater” with deep-cleanings or cash bans, Thompson writes. But “pandemic or no pandemic, you should wash your hands,” he adds: https://www.theatlantic.com/ideas/archive/2021/04/end-hygiene-theater/618576/.
ENTERTAINMENT:
14)





15)


16) SOUND ON:


17)


EARTH DAY:
18) Check out what young people in Argentina, Colombia, and Kuwait are doing about climate change and the health of the planet (by Mark Fischetti at Scientific American, 4/15/21): https://www.scientificamerican.com/article/youth-leaders-for-climate-justice-say-we-are-ready-to-work/.
————
CHECK OUT THESE CORONAVIRUS NEWSLETTERS: Patrice Peck’s “Coronavirus News for Black Folks;” Betsy Ladyzhets’ “Covid-19 Data Dispatch.”
COVID-19 VACCINE COMPARISON TABLE: Here’s the latest such table by Your Local Epidemiologist Katelyn Jetelina (4/2/21): https://yourlocalepidemiologist.substack.com/p/vaccine-table-updated.
THE PUBLISHING INDUSTRY: A lot of online media content is free during the pandemic, as a public service, but publishing, like many industries, is struggling. If you have the means, please subscribe to or purchase worthy publications.
TAG ME: Please reply to this email to send feedback and/or good SARS-CoV-2 or COVID-19 science coverage that you’ve read, written, or produced in English, Spanish, French, etc.
Thanks to my patrons!
Love/In friendship, Robin